











HTML
-
Hemorrhagic fever with renal syndrome (HFRS) is an endemic zoonosis in Eurasia [7]. It's a disease caused by viruses of the family Bunyaviridae, genus Hantavirus.Worldwide, several different human pathogenic Hantaviruses are known. Hantaviruses are transmitted to humans through aerosols of excreta from small mammals, mainly rodents that have had silent lifelong-infections [4, 5]. These viruses cause hemorrhagic fever with renal syndrome (HFRS) in Asia and Europe and Hantavirus pulmonary syndrome (HPS) in America [6, 7]. Actually, there are some hantaviruses associated with development of HFRS: Hantaan virus (HTNV), Dobrava/Belgrade virus (DOBV), Seoul virus (SEOV), Puumala virus (PUUV) and Saaremaa virus (SAAV), while HPS is caused by Sin Nombre (SNV) and related viruses [6, 7].
In Albania, the first cases were confirmed in 1985 [2]. From this time onwards, especially during the last decade, reported cases have been very rare. HFRS is endemic in the Balkan Peninsula, where sporadic cases or outbreaks have been reported [3, 5].
The following case report demonstrates the general difficulties associated with the diagnosis of HFRS by Dobrava virus infections in an area where the disease is sporadic. This is a serologically documented case of HFRS from Macukulli village (district of Burrel in Albania), associated with abdominal effusion and orchitis.
-
A 25-year old male woodcutter from Macukulli (Burrel), was admitted to the local hospital, and then was transferred to the tertiary hospital center, "Mother Teresa", Tirana. He presented a 5 days history of fever, chills, headache, hiccup, facial flushing, nausea and vomiting, as well as lumbar, testicular and abdominal pain.On admission he was febrile (39.2℃), somnolent but well oriented, hypotensive (systolic blood pressure 80 mmHg, heart rate 105/min), with conjunctivitis, abdominal tenderness in all quadrants, and an edematous painful right testicle. No hemorrhagic manifestations were found on skin examination. Results of laboratory examinations were as follows: white blood cell (WBC) count 9200/µL (range 4.0-10.0×103), with 79.1% neutrophils, red blood cells (RBC) 5.94×106/mm3 (range 4.2-5.8×106), hematocrit 43.4% (range 37.0-50.0), erythrocyte sedimentation rate (ESR) 30 mm/h, platelet count 58×103µL (range 150-400×103), creatinine 2.57 mg/dL (range 0.66-1.44), BUN 85 mg/dL (range 10.0-43.0), aspartate aminotransferase(AST) 163U/L (range 0-35), Alanine aminotransferase(ALT)111U/L(range0-45), C-reactive protein 85 mg/L (range 0-5); with other routine lab values within normal range. Urine analysis found a nonselective proteinuria with a total loss of 6.6 g/L and microscopic hematuria. Free abdominal fluid was seen on abdominal ultrasound. No pulmonary involvement was seen in physical examination and X-ray. He was treated with Doxycycline 100 mg twice daily for possibility of leptospirosis, rickettsiosis or other infective diseases with the same clinical aspects. Two days after admission, the patient became afebrile and normotensive. On the first three days after admission, intravenous administration of 5-7 L of fluid was necessary to sustain blood pressure. For four days post admission, the patient was oliguric with urine volume less than 0.5mL/kg/hr. He became polyuric on day 5, with urine output of 200-250mL/h and gradual recovery of renal function (Fig 1). Platelet count was elevated to normal on day 5 after hospital admission (Fig. 1). Serological diagnosis was confirmed by the Laboratory of Virology, Institute of Public Health (IPH), Tirana, Albania. The blood was tested according to the rules for transportation of contagious substances for Hantavirus profile 1 (EUROLINE). Blood samples were collected from the patient during the acute phase (on admission). The patient was tested for Crimean-Congo of hemorrhagic fever (CCHF), leptospirosis, brucellosis, rickettsioses and Gonococci and Chlamydia trachomatis infections, all of which tested negative, whereas serological testing for hantavirus infection resulted positive for IgM antibody for Dobrava virus; HBsAg resulted positive too. Further testing confirmed that our patient was a carrier of Hepatitis B virus but didn't have an acute or chronic hepatitis B infection that could explain the presence of abdominal fluid. The patient was discharged in good physical condition on day 15 after admission.
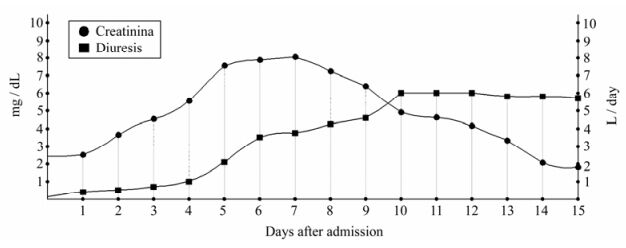
Figure 1. Progression of renal function parameters
-
The above described clinical case is an example of the difficulties in diagnosis of HFRS, especially in areas where the disease is not endemic. Similar cases have occurred in Scandinavian countries and Russia, especially when HFRS is not generally recognized [12].
Macukulli is a hilly-mountain area with altitude between 608-1191m in northeastern Albania. The first case of HFRS in Albania was diagnosed in 1985 in Northern part of the country. During the years 1985-1987, 31 cases were diagnosed [2]. Twenty percent of cases, mainly in North of the country, showed a severe clinical syndrome with renal failure and impairment of liver function. The cases were diagnosed from March to August in 6 districts and at high altitudes 700m above sea level in the North, South-East and South of the country. Three other cases were identified from 2003-2006 from May to August in high altitudes in the North and another case in lower altitudes in the South-West. In 2008 and 2009, two further cases were diagnosed in December, at both high and low altitudes [2].
During recent years, it has become clear that infections from Dobrava virus are occurring not only in the Balkan Peninsula but also in other European countries [3-6, 9-11].
The epidemiology of Hantavirus is closely linked to the ecology of their principal host and interactions between rodents and humans [8, 9]. Apodemus flavicollis is the most common and widespread small mammal in Albania, except for coastal lowlands, where its habitats have been heavily degraded by agriculture and in these regions Apodemus sylvaticus predominates. The typical habitat of Apodemus flavicollis is forest and woodland: oak forests at 150-860 m above sea level, beech forests at 1100-1700 m above sea level, and mixed forests, pine stands and fir forests at altitudes 730-1350 m.
Transmission of the virus to man occurs through inhalation of infected animals excreta, i.e. urine, feces and saliva [4]. Though the aerosol route of infection is undoubtedly the most common means of transmission among rodents and to humans, virus transmission by bite occurs among rodents and may also result in human infection. Transmission between human beings has not been documented. Occupation is a dominant factor, with animal trappers, forestry workers, farmers and military personnel at highest risk. Working with wood piles and cleaning long abandoned buildings seem to significantly increase the risk for Hantavirus infection [4, 6, 8, 9, 12]. Epidemiological investigations have linked viral exposure to activities such as heavy farm work, threshing, sleeping on the ground, military exercises, and lower socioeconomic status [3, 5]. In contrast to previous cases which are presented during the spring and summer periods this new case was admitted in December with an infective source originating at more than 700m above sea level. Usually during this period the originating area is snow-clad but global climate changes are probably altering the typical seasonal presentation of infections from DOBV making possible infections during winter time. HFRS infection is more common in males than in females [11]. The incubation time is estimated to be from 4 -42 days [3, 4]. The physiological derangement in HFRS is vascular dysfunction, manifested by impaired vascular tone and increased vascular permeability [11].This maybe could explain the abdominal liquid and orchitis in our patient. HFRS is manifested as mild, moderate, or severe disease, depending in part on the causative virus. Case-fatality rates in Balkan from HFRS are as high as 12% [6].
Our patient had renal failure on admission (fifth day of the disease) which peaked on days 5-7 after admission. In classical cases, thrombocytopenia is most severe by day 9 and begins to resolve thereafter. Our patient presented with decreased platelet count on admission with the lowest count the next day and increasing platelet count thereafter. Elevated hepatic enzymes are common but do not reach high levels. Gastrointestinal symptoms are also common in Hantavirus infections. Because the clinical features of Dobrava virus infections are not pathognoonic, laboratory work-up is essential for making the diagnosis.
-
We think that this case is the first case of HFRS by Dobrava virus infection complicated by orchitis. Areas of Dobrava virus endemicity in Western and Central Europe are not well defined, and Dobrava virus infections may be more common than expected. Global climate changes are altering the seasonality of Dobrava virus infections making probable wintertime infections.

 DownLoad:
DownLoad: