











HTML
-
Human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (AIDS) remain major public health problems in China, where approximately 780, 000 people currently live with HIV, according to the 2012 China AIDS Response Progress Report. Suzhou was an early epidemic region in Jiangsu province and the current situation of HIV-1 prevalence is complicated. In the late 1980s, a labor force returning to Suzhou from Asia and Africa contributed to an early HIV-1 epidemic in the region. The first case of HIV-1 in Suzhou was identified by a sexually transmitted disease clinic in 1992 (Xia et al. 1993). Suzhou later attracted migrant populations, complicating the HIV-1 subtypes circulating in the region. In 1998, an immigrant from Xinjiang province was diagnosed as the first case of HIV-1 acquired by intravenous injection in Suzhou (Shao et al. 1999a). According to HIV epidemic surveillance data collected in Jiangsu province since 2011, Suzhou is now one of five cities in Jiangsu with a severe HIV-1 epidemic and it has the second-highest incidence of HIV and AIDS (Ding et al. 2012). By the end of 2012, 1, 588 cases of HIV-1 were reported in Suzhou (Fu et al. 2013). A patient survey revealed that HIV spread in Suzhou from 1992 to 1997 via people returning from abroad. After 1998–2001, several cases were reported among drug users, commercial blood donors, and blood-product users. Since 2002, the number of cases has rapidly increased annually and shifted from high-risk to normal populations. Sexual contact and intravenous injection have gradually became main transmission routes (Zhao et al. 2005). Notably, the infection rate among men who have sex with men (MSM) has been increasing particularly rapidly recently (Fu et al. 2014). Despite these data, HIV-1-related molecular epidemiological information in Suzhou remains minimal, aside from a recent investigation of HIV-1 diversity in Suzhou and Suqian from 2011–2013 (Qin et al. 2016). However, only 24 sequences isolated in Suzhou were characterized, which was insufficient for adequate statistical analysis.
Here, we analyzed the subtype, genetic variation, and transmission characteristics of 261 HIV-1-positive samples collected by the local Center for Disease Control (CDC) in Suzhou in 2009 and 2012–2014. HIV antibodies were testedat the Suzhou CDC using an ELISA kit (Wantai BioPharm, Beijing, China) and western blotting (HIV1 + 2; MP BiomedicalAsiaPacific Pte., Ltd., Singapore). Althoughmost samples used were acquired from hospital (n = 104; 39.8%) and follow-up populations (n = 75; 28.7%), some originated from voluntary counseling and testing (VCT) attendees (n = 37; 14.2%), prisoners (n = 25; 9.6%), blood donors (n = 11; 4.2%), and people undergoing medical examinations (n = 9; 3.4%), suggesting that HIV-1 has begun to spread from high-risk populations to the general population in Suzhou (Supplementary Table S1). A previous study reported that HIV-1 tended to infect younger and older people (Qin et al. 2016). We verified this trend in Suzhou and found that the age of patients with HIV-1 ranged from 2 to 75 years, with 10 patients ≤ 18 (3.8%) and 41 patients ≥ 50 years of age (15.7%). Patients aged 19–29 years accounted for a large proportion of our HIV-1-infected cohort (n = 108; 41.4%), most likely because of sexual activity. Additionally, among the 261 patients, most cases were due to sexual contact (n = 226; 86.6%), including 170 cases of heterosexual contact (65.1%, with eight cases of transmission between spouses) and 56 cases of homosexual contact (21.5%), followed by 29 cases involving intravenous drug use (11.1%) and six cases of maternal vertical transmission (2.3%). Therefore, information regarding AIDS prevention and intervention measures should be provided to high-risk populations likely to engagein sexual contact, such as sex workers and MSM, in order to control the spread of HIV-1. Viral RNA was extracted from 140 μL plasma; HIV-1 cDNA was obtained by reverse transcription PCR, followed by amplification of the env, gag, and pol gene fragments using nested PCR, as previously described (Liao et al. 2007; Song et al. 2007; Stoeckli et al. 2000). The env C2V3 region of gp120 (HXB2; 7002–7668 nt), the p17–p24 region of gag (HXB2; 836–1507 nt), and a pol fragment (HXB2; 2147–3462 nt) were selected for amplification. HIV-1 subtypes were analyzed using HIV BLAST on the Los Alamos HIV Database (https://www.hiv.lanl.gov/content/sequence/BASIC_BLAST/basic_blast.html). BioEdit 7.0 (http://www.mbio.ncsu.edu/BioEdit/bioedit.html) was used for sequence editing and ClustalX (www.clustal.org/clustal2/) was used for sequence alignments. MEGA 7.0 (http://www.megasoftware.net/) was used for phylogenetic analysis of aligned sequences using the neighbor-joining method and bootstrap testing (1000 replicates), with bootstrap values displayed on the corresponding node of the phylogenetic tree (>70%).

Table Supplementary Table S1. Demographic information of patients with HIV-1 in Suzhou
A total of 169 env, 235 gag, and 216 pol sequences were obtained. Genotype analysis according to the env and gag sequences detected two subtypes (B and C) and three circulating recombinant forms (CRFs; CRF01_AE, CRF07_BC, and CRF08_BC).Ofthese, CRF01_AE was the mostcommon (52.1%), followed by CRF07_BC (30.3%), CRF08_BC (8.4%), and the B subtype (8%), while the C subtype accounted for only 1.2% of the samples (Fig. 1A). However, no new recombinant forms were found in our study. Notably, HIV-1 genotype dynamics monitoring over several years revealed that although CRF01_AE was the most common form, CRF07_BC became more predominant over time (Fig. 1A). This result was consistent with a previous study, which identified 56% CRF01_AE (n = 13) and 26.1% CRF07_BC (n = 7) circulating in Suzhou (Qin et al. 2016). Because of our large sample size, we also detected the B subtype, which was not detected in the previous study. Similarly, the genotype distribution in different sample groups indicated that CRF01_AE, followed by CRF07_BC, were the most common in all groups, except for the prisoners group, in which CRF07_BC was detected more often than CRF01_AE. CRF01_AE (n = 8) and CRF08_BC appeared only in the physical examination group (Supplementary Figure S1). CRF01_AE reportedly circulates by sexual transmission (An et al. 2012). Consistent with previous results, the major transmission route of HIV-1 in Suzhou was sexual contact, including heterosexual and homosexual routes, and CRF01_AE was the predominant subtype. CRF07_BC was identified as the major subtype in intravenous drug users from Guangxi, Yunnan, and Xinjiang (Shao et al. 1999b). In our study, CRF07_BC strains circulated not only in intravenous drug users, but also among populations reporting sexual contact, suggesting that this strain was also transmitted sexually in Suzhou. The B subtype, originally isolated in Yunnan province, is now distributed across the country (He et al. 2012); sexual transmission rather than blood donations or transfusions currently represents the predominant transmission route of the B subtype (Ng et al. 2013). Moreover, we observed low HIV-1 transmission rates between spouses (n = 8; 3.1%) and from mother to child (n = 6; 2.3%). The MSM population has attracted increasing attention regarding HIV transmission (He et al. 2006). HIV-1 risk increases with unprotected sexual intercourse, multiple sex partners, commercial sex consumption, and bisexual behavior; compared with other high-risk populations, the MSM population is young, highly educated, and private (Sun et al. 2016). In our study, the MSM group accounted for 21.3% (n = 56) of the samples; CRF01_AE was its main subtype, while CRF07_BC and B were also present. One 8-member cluster was identified in the MSM group in the phylogenetic trees; it was associated with CRF01_AE env, gag, and pol (Fig. 1B). These data indicate that members of the MSM group are closely related and prone to cross-infection. Genetic distance calculations for the major subtypes and CRFs revealed that the genetic distance of the B subtype circulating in Suzhou was greater than that of other subtypes (Table 1). The genetic distances for the HIV-1 B subtype env, gag, and pol regions were 0.187 ± 0.035 (P < 0.01), 0.071 ± 0.020 (P < 0.05), and 0.049 ± 0.018 (P < 0.05), respectively, indicating that the HIV-1 B strain was introduced into Suzhou via complex routes. The CRF01_AE strains in the MSM group exhibited lesser distance than the CRF01_AE strains in Suzhou (P < 0.01) (Table 1). The genetic distances of gag and pol of the 8-membercluster werelesserthanthoseofthe MSM group (P < 0.01) and there was no significant difference in the distance of the env region between these two groups (P > 0.05), indicating high convergence of HIV-1 strains in these groups. It is important to determine the factors affecting HIV-1 spread to reduce the risk of HIV-1 transmission and infection in the MSM population.

Figure 1. A Distribution of HIV-1 subtypes or CRFs in Suzhou from 2009–2014. The env, gag, and pol genes from 261 HIV-1 antibodypositive serum samples were amplified and sequenced. These sequences were compared with corresponding subtype reference sequences in an HIV database (www.lanl.hiv.gov/index) and subtypes were determined according to env and gag. B Phylogenetic trees based on the env, gag, and pol genes of CRF01_AE strains circulating in MSM. The tree was generated using 37 CRF01_AE strains isolated from MSM with the neighbor-joining model and maximum composite likelihood method in MEGA 7.0. The bootstrap method was used for the phylogeny test. The number of bootstrap replications was 1000. Bootstrap values greater than 70% are displayed on the corresponding node. The genome sequence of the env, gag, and pol genes of CRF01_AE strains circulating in MSM were deposited in the GenBank with the accession number MG893938–MG893974, MG893975–MG894011, and MG894012–MG894048, respectively. The CRF01_AE reference sequence was 01_AE_TH.90.CM240. The cluster containing the same eight members is designated by black solid triangles in the env, gag, and pol phylogenetic trees.
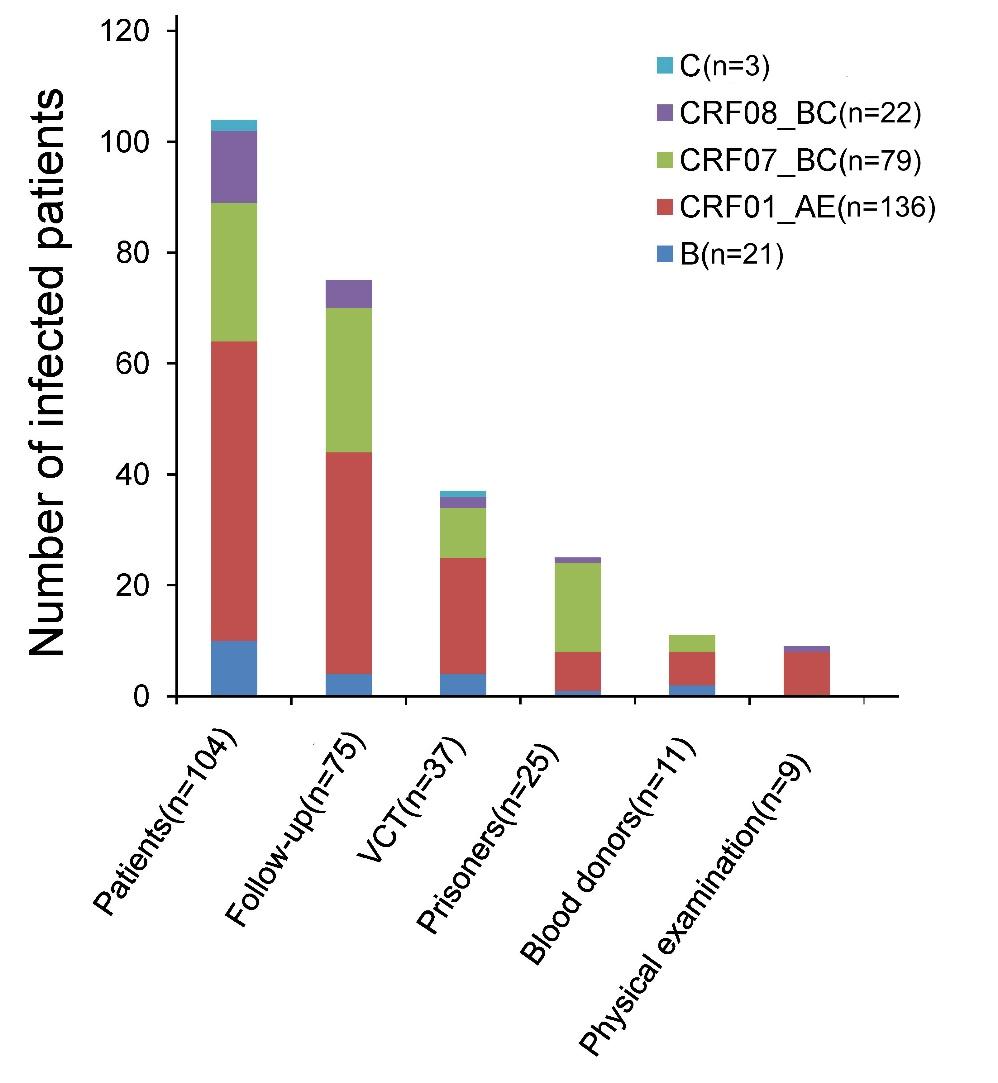
Figure Supplementary Figure S1. HIV genotype distribution in different risk groups

Table 1. Gene distance analysis of major HIV-1 strains in Suzhou
In summary, multiple HIV-1 subtypes are circulated mainly by sexual transmission in Suzhou, with CRF01_AE representing the dominant strain. The CRF07_BC strain is spreading from intravenous drug users to populations engaging in sexual contact. Additionally, the source of the B subtype in Suzhou is complicated, which may explain the high level of variation in this subtype. An 8-member cluster was found in the phylogenetic tree of MSM group CRF01_AE samples; therefore, intensive monitoring of high-risk sexually active populations should be conducted. These findings further our understanding ofincomingsources of HIV-1 strains in Suzhou and could improve HIV/AIDS prevention and control.
-
We gratefully acknowledge the contribution of the HIV-1 patients who participated in this study and also wish to thank the staff of the local CDC for recruiting participants, collecting samples, and technical assistance. This work was supported by grants from the Open Research Fund Program of the State Key Laboratory of Virology of China (2017IOV003), the Health Department of Jiangsu Province (Y2013062), and Suzhou Science Technology Bureau (SYS201452) and in part by grants from the National Science Foundation of China (NSFC) (81101257) and the Natural Science Foundation of Heilongjiang Province (H201355).
-
The authors declare that they have no conflicts of interest.
-
Animal and Human Rights Statement was obtained from all patients for whom identifying information is included in this article.

 DownLoad:
DownLoad: