








HTML
-
Crimean-Congo hemorrhagic fever (CCHF), first described in the mid-20th century in Crimea and later in the Congo, is a zoonotic viral infection that is asymptomatic in animals but a serious threat to humans (Ergonul O, 2006). Currently, it is one of the most widely distributed viral hemorrhagic fevers reported in parts of Africa, Asia, Eastern Europe, and the Middle East (Ergonul O, 2012). Infection in humans usually occurs via a tick bite or from contact with the blood or body fluids of infected livestock and human patients (Mardani M, et al., 2007). Human infections start with nonspecific febrile symptoms, but may progress to a serious hemorrhagic syndrome with consequential high mortality rates (Ergonul O, 2006). The widespread geographical distribution of the virus with its ability to produce fatal human disease is presently a significant public health concern. Moreover, with the continuing globalization of the world and changing climate and ecology, the prevalence of the disease is likely to spread into new regions in the near future (Leblebicioglu H, 2010; Purnak T, et al., 2007). Thus, instead of remaining a local health problem, CCHF should be recognized as a global health threat. In this review, all aspects of CCHF are considered in light of the current literature.
-
The causative agent, CCHF virus (CCHFV), is a negative sense, single-stranded RNA virus in the genus Nairovirus, family Bunyaviridae (Bajpai S, et al., 2011). The genome is circular and includes small (S), medium (M) and large (L) segments. The L segment encodes the RNA polymerase; the M segment encodes the envelope proteins; and the S segment encodes the nucleocapsid protein (Hewson R, et al., 2004). Although early serological studies suggested modest differences between strains of CCHFV, nucleic acid sequence analysis has revealed broad genetic diversity, mainly between viruses from different geographic regions (Deyde V M, et al., 2006). Phylogenetic analysis of the CCHFV strains showed that, based on S-segment sequences, they cluster in seven distinct clades (Table 1)(Anagnostou V, et al., 2009; Putilina N G, et al., 2011).The identification of distinct clades of CCHFV has important epidemiological implications and they can give clues about the source of infection during an outbreak and also aid in tracing the path of spread of imported cases (Appannanavar S B, et al., 2011). To this end, high levels of nucleotide and amino acid differences, common RNA segment reassortment and even RNA recombination have been recently described (Deyde V M, et al., 2006; Duh D, et al., 2008). This diversity underlines the necessity to determine the complete genome sequence of CCHF virus, from representative samples of all geographically distinct endemic areas. The antigenic differences among diverse clades should also be considered while choosing the target for vaccine development (Appannanavar S B, et al., 2011; Keshtkar-Jahromi M, et al., 2011).
Clades Geographic location Africa 1 Iran, Senegal Africa 2 Congo, Uganda Africa 3 Mauritania, Nigeria, South Africa Asia 1 Iran, Iraq, Madagascar, Oman, Pakistan, United Arab Emirates Asia 2 Central Asia, China, Kazakhstan, Tajikistan, Uzbekistan Europe 1 Albania, Bulgaria, Greece, Kosovo, Russia, Turkey Europe 2 Greece Table 1. Geographic distribution of CCHFV based on phylogenetic analysis of the S segment
-
CCHFV generally circulates unnoticed in nature in an enzootic tick-vertebrate-tick cycle. The genus Hyalomma, particularly H. marginatum marginatum, is considered as the principal tick vector (Bajpai S, et al., 2011). But the virus has also been isolated from other ticks of other genera (e.g. Dermacentor, Rhipicephalus) which may help to explain the wide geographical distribution of the disease (Tekin S, et al., 2012). These vectors achieve both trans-ovarial and trans-stadial transmission of the virus, further contributing to circulation of the virus in nature by remaining infected during their developmental phases and by passing to the next generation (Appannanavar S B, et al., 2011). Numerous domestic and wild vertebrates (cattle, sheep, goats, hares, hedgehogs etc) serve as a source of blood for the ticks. Smaller wildlife species usually harbor the tick vectors that are at immature stages. These small animals are believed to act as amplifying hosts and sustain the virus in nature (Appannanavar S B, et al., 2011). Infections in animals generally result in unapparent or subclinical disease. Exceptionally, birds are observed to be refractory to CCHFV infection but are thought to play a role in the transportation of CCHFV infected ticks (Jameson L J, et al., 2012). Human mobility (including military movements), movements of mammal wildlife, trade in livestock and animal products are possible pathways additional to migratory birth movements that can distribute CCHFV worldwide.
CCHF in human is mainly an occupational disease; veterinarians, agricultural workers and slaughterhouse workers in endemic areas are people most at risk to contract the infection. Humans become infected through the skin and mucosa. Tick bites, crushing a tick with exposed skin and contacting body fluids or tissues of an infected animal are the potential modes of zoonotic transmission (Mardani M, et al., 2007). In addition to zoonotic transmission, human infection can also be acquired from exposure to infected blood and body fluids of a patient. Nosocomial transmission and outbreaks have also been reported in many regions (Mardani M, et al., 2007). Aerosol transmission and horizontal transmission have been suspected in a few cases but cannot be proved conclusively (Saijo M, et al., 2004). The enzootic cycle and transmission of CCHFV are outlined in Fig. 1. The disease has a seasonal pattern, related to the increased activity of ticks, and peaks between spring and early autumn(Leblebicioglu H, 2010).

Figure 1. Enzootic cycle and transmission mode of CCHFV.
The geographic range of CCHFV is the most extensive among the tick-borne viruses that affect human health (Ergonul O, 2006). Since CCHF was first discovered in the Crimea region and Congo Basin, the disease has been reported in many regions. Currently, over 50 countries in Africa, Asia, the Middle East and Europe have been recognized as endemic or potentially endemic regions (Fig. 2). Countries reporting outbreaks and increasing numbers of cases include Turkey, Greece, Bulgaria, Kosovo, Georgia, the Russian Federation, Kazakhstan, Tajikistan, Iran, Iraq, United Arab Emirates, Saudi Arabia, Albania, Pakistan, Afghanistan, Mauritania, Kenya, Uganda, Senegal, South Africa and also India (Bakir M, et al., 2005; Chinikar S, et al., 2010; Humolli I, et al., 2010; Kebede S, et al., 2010; Leblebicioglu H, 2010; Mourya D T, et al., 2012). Limited serological evidence also suggests that CCHF might also occur in additional areas throughout the world (Heyman P, et al., 2010; Sanchez-Seco M P, et al., 2005; Xia H, et al., 2011), which are indicated in Fig. 2.
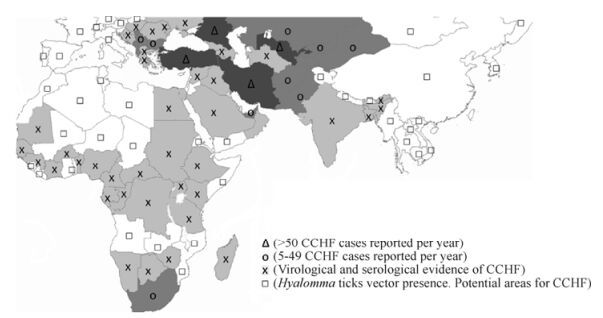
Figure 2. Geographic distribution of CCHF. Data source: World Health Organization (WHO); The Figure was created based on a map available at http://www.who.int/csr/disease/crimean_congoHF/Global_CCHFRisk_20080918.png
-
Owing to the limited number of studies, there are still some uncertainties regarding the pathogenesis of CCHF but analogy with other arthropod-borne hemorrhagic fevers may provide insight into the mechanisms. CCHFV undergoes some level of replication at the site of inoculation and afterward spreads via the lympho-hematogenous pathways to lymphoproliferative organs, mainly the liver, where it replicates. The pathogenic capability of the virus to infect the immune cells protects the virus from phagocytosis and eventually hinders the host immune response, thereby enhancing the spread of the virus (Chinikar S, et al., 2010; Geisbert T W, et al., 2004). Endothelial involvement also has an important role in CCHF pathogenesis. The endothelium is targeted in two ways—directly by virus infection and/or indirectly by virus-mediated host-derived soluble factors that cause endothelial damage (Ergonul O, 2006). Endothelial injury resulting in stimulation of platelet aggregation and degranulation eventually contribute to the occurrence of hemorrhagic diathesis (Bodur H, et al., 2010). On the other hand, infection triggers the inflammatory cascade by the release of cytokines, pro-coagulants and other inflammatory mediators (Papa A, et al., 2006). This inflammatory storm may result in the development of Disseminated Intravascular Coagulation (DIC) which is a symptom of severe disease (Ergonul O, et al., 2006). In a recent study, reactive hemophagocytosis was also reported during the course of an infection (Erduran E, et al., 2010). All of these processes contribute to development of microvascular instability and impaired hemostasis which are the hallmarks of the infection. Immunological and inflammatory changes were also observed in a CCHFV infected STAT-1 (Signal Transducer and Activator of Transcription 1) knockout mouse model which demonstrated the crucial role of interferon in controlling viral replication (Bente D A, et al., 2010).
-
There are four distinct phases during the course of the disease: incubation phase, pre-hemorrhagic phase, hemorrhagic phase and convalescence phase. The incubation period of the disease is, on average, 5-6 days but may be as low as 2-3 days or as long as 2 weeks, possibly depending on the exposure type, virulence and viral load (Ergonul O, 2006). The pre-hemorrhagic phase of CCHF is characterized with influenza like illness. Sudden onset of high fever, chills, headache, photophobia, myalgia, arthralgia, conjunctivitis and dizziness are the characteristic symptoms. Nausea, abdominal pain, non-bloody diarrhea, rash and neuropsychiatric signs are other symptoms that are not infrequently observed in this period (Bakir M, et al., 2005). The pre-hemorrhagic phase continues for several days and is followed by the hemorrhagic phase that develops abruptly and is short in duration (usually 2-3 days). In this stage, patients may show signs of progressive hemorrhagic diathesis, such as mucous membrane and conjunctival hemorrhage, petechiae, epistaxis, hematuria, hematemesis, melena and intracerebral hemorrhage. Patients usually develop DIC, circulatory shock and multiorgan dysfunction syndrome (MODS) before death which occurs 1-2 weeks after the onset of symptoms (Ergonul O, 2006). In surviving patients, the convalescence period is commonly characterized by prolonged and pronounced generalized weakness (Ergonul O, et al., 2004). Other complaints such as headache, dizziness, nausea, appetite loss, temporary hair loss, polyneuritis, memory problems, hearing loss and vision problems have been reported to accompany this phase of the disease (Ergonul O, 2006). However, the clinical course of the disease is not always as described, hence the duration and manifestations during the phases may vary from patient to patient. Such circumstances are usually recognized in the hemorrhagic phase of the disease. Despite an increased risk for bleeding, it is not always the case in this phase of the disease (Ertugrul B, et al., 2009). In such cases the clinical course is usually perceived as influenza like infection. Moreover, some field studies conducted in endemic area reported seropositive populations indicating previous infections without apparent clinical symptoms (Ertugrul B, et al., 2012). Accordingly, it is claimed that some individuals may be subclinical during the course of infection (Bodur H, et al., 2012). Additionally, the clinical course of the disease has also been reported to be milder among children (Tezer H, et al., 2010)
-
Thrombocytopenia, leucopenia and elevated levels of aspartate aminotransferase (AST), alanine aminotransferase (ALT), lactate dehydrogenase (LDH), and creatinine phosphokinase (CPK) are consistent laboratory features of CCHF. Abnormal laboratory observations usually start at beginning of the infection and become most prominent during the hemorrhagic phase (Ergonul O, 2006). Abnormal coagulation tests such as increased bleeding time, prothrombin time and activated partial thromboplastin time, decreased fibrinogen and increased fibrin end products might be detected during the 3rd phase of the infection.
-
Early diagnosis is important, both for the outcome of the patient and to avoid further transmission of disease. In patients with symptoms suggesting CCHF, a detailed history is necessary for a risk assessment. History of travelling to endemic areas, tick bite and exposure to body fluids of livestock or human patients can support the diagnosis. In such cases, after ensuring preventive measures, a laboratory diagnostic workup should be started rapidly. Methods of diagnosis include antibody detection, antigen detection, polymerase chain reaction (PCR) and virus isolation (Vanhomwegen J, et al., 2012).
Antibody detection by serological tests is in widespread use for the diagnosis of CCHF. Enzyme-linked immunosorbent assay (ELISA), indirect immunofluorescence assay (IFA), hemagglutination inhibition, complement fixation, and immunodiffusion are the various techniques for antibody detection in order of decreasing sensitivity. Owing to the low cost and ease of application, ELISA is the most common test for the antibody detection with a sensitivity of more than 90% (Putilina N G, et al., 2011). It detects CCHFV-specific IgM, or a four-fold rise in IgG titers in paired acute and convalescent sera, both of which are diagnostic for the disease (Burt F J, et al., 1994). However, as antibody levels only become available from about the sixth day of the illness, this test may not be effective in the initial stage of infection. Specific IgM declines to undetectable levels by about 4 months post-infection, but IgG remains detectable for several years. On the other hand, patients with fatal disease may not produce a measurable antibody response similar to patients in the first few days of illness, and in these individuals diagnosis should be achieved by demonstration of viral antigen by ELISA, detection of viral nucleic acid by reverse transcriptase PCR (RT-PCR), or isolation of the virus (Mardani M, et al., 2007). Viral antigens can also be identified with ELISA (Saijo M, et al., 2005). Although this test is less sensitive than PCR, it can detect nucleoproteins in acute sera of CCHF patients. The presence of anti-CCHFV IgG decreases the sensitivity of the ELISA, possibly due to competition with monoclonal antibodies. However, the method may be useful for the diagnosis of acute stage of CCHF, especially in areas where the laboratories are not equipped with RT-PCR testing capabilities. Although not frequent, cross-reactivity by ELISA with the closely related nairovirus (Hazara, Nairobi sheep disease, Dugbe viruses etc) has been reported (Zeller H, 2007). PCR is a very specific, sensitive and rapid method for the identification of CCHFV as well as different lineages (Ibrahim S M, et al., 2011). This method also enables quantification of viral load which may have prognostic value. Techniques usually combine the reverse transcription step with specific amplification thereby minimizing the risks of contaminations (Drosten C, et al., 2002). Moreover, automated real-time assays have higher sensitivity and specificity, a lower contamination rate and are more rapid than conventional RT-PCR (Atkinson B, et al., 2012). However, isolation of CCHFV from blood, plasma or tissues is the most definite test. This technique is of use during the first five days of illness but it is of limited value as virus isolation takes longer time (2-5 days), lacks sensitivity and can only detect high concentrations of the virus (Shepherd A J, et al., 1986). Additionally it necessitates access to a biosafety level 4 (BSL-4) laboratory which is not available in most areas.
-
Detailed patient history and examination are of critical importance as there are a number of diseases presenting similar clinical features that should be ruled out before diagnosis. Firstly, other hemorrhagic fevers should be considered according to the origin of patient and risks of potential exposure (Ergonul O, 2012). These include Alkhurma in the Middle East and Africa; Omsk hemorrhagic fever in Russia; Kyasanur Forest disease in India; Lassa, Ebola, Marburg and Rift Valley fever in Africa; yellow fever in Africa and America; hantavirus and dengue in locations worldwide (Marty A M, et al., 2006). The differential diagnosis should also include rickettsiosis, leptospirosis, typhoid fever, malaria, meningococcemia, borreliosis, ehrlichiosis, Q fever and influenza.
-
Treatment is mainly supportive in nature with careful maintenance of hemodynamic status. Medications (aspirin etc) and interventions (intramuscular injection etc) that facilitate bleeding should be avoided. In case of requirement of fresh frozen plasma, thrombocytes and erythrocyte preparations should be infused to the patient. Although there is no FDA approved specific antiviral therapy for CCHF, ribavirin has been commonly used over the years with promising results. But, due to ethical concerns, there is no controlled randomized human study that shows conclusive evidence of the benefits of using ribavirin to treat CCHF. Nevertheless, in-vitro studies support the use of ribavirin as it has been shown to inhibit viral activity of CCHFV and substantially reduce infant mouse mortality by extending the mean time to death (Tignor G H, et al., 1993; Watts D M, et al., 1989). Also, uncontrolled human studies on both sporadic and outbreak cases reported some anecdotal benefits by ribavirin, mainly associated with early treatment (Cherenov I V, et al., 2012; Ergonul O, et al., 2004; Fisher-Hoch S P, et al., 1995; Izadi S, et al., 2009; Mardani M, et al., 2007; Sharifi-Mood B, et al., 2009; Tasdelen Fisgin N, et al., 2009). However, the use of ribavirin for CCHF treatment remains an issue of controversy as there are also studies that showed no difference in case of fatality rates (Bodur H, et al., 2011; Duygu F, et al., 2012; Elaldi N, et al., 2009; Koksal I, et al., 2010; Ozkurt Z, et al., 2006). Recently published systematic reviews and meta-analysis on the use of ribavirin for CCHF concluded that there is no clear message of benefit available from the current data on ribavirin as observational data are contradictory (Ascioglu S, et al., 2011; Soares-Weiser K, et al., 2010). However, ribavirin could potentially have benefits in the treatment of CCHF and these above results clearly indicate the need for a well designed randomized controlled trial in the context of good quality supportive care (Soares-Weiser K, et al., 2010). Nevertheless, until precise data are available against its usage, ribavirin should not be completely ruled out as a treatment option, especially at the earlier phase of severe CCHF. Because of its potential benefits, it is also recommended by the World Health Organization (WHO) with a schedule of 30 mg/kg loading dose, followed by 15 mg/kg every 6 h for 4 days, and finally 7.5 mg/kg every 8 h for 6 days.
Antibodies to CCHFV are typically not present within 5-7 days after the onset of illness, and dying patients do not usually produce a measurable antibody response (Ergonul O, 2008). The lack of antibody development encouraged the use of immunotherapy via passive transfer of CCHF survivor convalescent plasma (Kubar A, et al., 2011; Vassilenko S M, et al., 1990). Although a favorable outcome was suggested, definitive evidence regarding their effectiveness is lacking. Further well designed studies are required to clearly establish the benefit of this treatment. Recombinant or natural interferon is another promising treatment opportunity for CCHF but, despite in vitro and animal models which have shown the antiviral activity of interferon against CCHFV, there are no clinical data to support its use yet.
-
The average case fatality rate of CCHF is 30-50%, but mortality rates from 2% to 80% have been reported in various studies (Chinikar S, et al., 2010; Mofleh J, et al., 2012; Whitehouse C A, 2004; Yen Y C, et al., 1985). The mortality rate of nosocomially acquired CCHF is usually higher than cases acquired from tick bites (Whitehouse C A, 2004). This is supposed to be the result of higher viral load which is indicative of disease prognosis. In CCHF, mean virus titers are significantly higher in fatal compared to nonfatal cases with fatal cases generally exceeding 108 genomes /ml plasma (Cevik M A, et al., 2007). Mortality rates may also differ according to the geographic location of the disease. Although rapid and effective healthcare availability in geographical regions is the main determinative of mortality rates, diversity in lineage virulence may have an additional role in the prognosis. On the other hand, hemorrhagic manifestations, confusion, advanced age, laboratory evidence of frank DIC, marked elevation of previously mentioned biochemical and coagulation blood tests, as well as thrombocytopenia are all reported predictors of fatal outcome (Bakir M, et al., 2012; Ozkurt Z, et al., 2006). Recent studies have also proposed a correlation between increased case mortality and high levels of C-reactive protein (CRP), D-Dimer and, C-type natriuretic factor (CNP) (Ozturk B, et al., 2012; Turkdogan K A, et al., 2012). But each of these prognostic indicators needs to be confirmed in larger case studies.
-
Although measures that aim to limit the spread of the virus through ticks and infected animals (including acaricide application and implementation of a quarantine period for animals brought from CCHF infested areas) are critical steps in prevention, personal protection is presently the most effective way to avoid infection. For the individual living in or travelling to endemic areas, use of efficient protective precautions against tick bite and minimizing animal contact are the best means to avoid infection. Precautions to keep away from tick bites include tick repellents, environmental modification (insecticides, brush removal etc), avoiding regions with high tick populations and regular examination of clothing and skin for ticks. People who are at risk of exposure to potentially infectious animals should take precautions to protect themselves (gloves and other protective clothing) to prevent skin and mucosa contact with infected tissue or blood. In case of caring for human patients strict universal precautions should be observed (Bajpai S, et al., 2011). These recommendations include patient isolation, barrier nursing and the use of gloves, gowns, face-shields and safety goggles (Leblebicioglu H, et al., 2012). Laboratory workers handling viral material are also at high risk of contracting the disease. Thus stringent biosafety precautions should be observed in the laboratory.
For individuals exposed to CCHFV, post-exposure prophylaxis may be considered for prevention of disease development. Those who have mucous membrane contact or have percutaneous injury with previously known infected blood or body fluids are potential candidates for prophylaxis. As discussed above, although there are no clear data regarding its efficacy as a prophylactic, some reports proposed ribavirin as a potentially beneficial agent in prevention of severe CCHF(Bangash S A, et al., 2003). Ribavirin as a potentially useful drug in prophylaxis is advised at a dosage of 200 mg twice daily for 5 days (Ergonul O, 2012), but this also needs to be established via a well designed studies in order to put forth precise recommendations.
Currently, there is no commercially available vaccine that is proven to be effective and safe for use in humans. An inactivated mouse brain vaccine was used for humans in Eastern Europe and the former Soviet Union (Papa A, et al., 2011). Although surveillance data suggested a reduction in the number of notified CCHF cases after the introduction of vaccination, data on vaccine efficiency have not been published (Whitehouse C A, 2004). In a recent Bulgarian study, a vaccine given to human volunteers was reported to elicit significant antibody production in 96.6% of these individuals (Keshtkar-Jahromi M, et al., 2011). All these data suggest that vaccine may be an efficient way to prevent the disease outbreak. But due to the method of preparation, the widespread usage of the current vaccine is limited. Therefore, a human vaccine that demonstrates efficacy in long-term in-field studies is required.
-
CCHF is a widespread disease and currently, over 50 countries in Africa, Asia, Middle East and Europe have been recognized as endemic or potentially endemic regions for CCHF. Methods of diagnosis include antigen/antibody detection, polymerase chain reaction (PCR) and virus isolation, but diagnostic methods need to be improved to detect early cases more precisely. Treatment is mainly supportive in nature with careful maintenance of hemodynamic status. Although definitive studies are not available, ribavirin is suggested to be effective especially at the earlier phase of the infection. However, randomized controlled trials in the context of good quality supportive care are needed to draw precise conclusions about its benefits. Use of universal protective measures is the best way to avoid infection. Although not definitely established with randomized trials, post-exposure prophylaxis with ribavirin may be considered for individuals with clear evidence of exposure to CCHFV to prevent disease development. Vaccination appears to be an effective way to prevent disease but safer human vaccines that show efficacy in long-term in-field studies are required for widespread application. Finally, effective communication between different regions and authorities will facilitate the exchange of information to improve surveillance, combat outbreaks and achieve better understanding of the factors impacting disease severity and fatality.


 DownLoad:
DownLoad:
{kind=link}