













HTML
-
Influenza is a contagious respiratory infection caused by influenza viruses. Influenza A and B are two types of influenza virus which is widespread and prevalent in human. Influenza can lead to 3 to 5 million severe infections and up to 650 000 people die of respiratory diseases linked to seasonal influenza each year (WHO 2017; Iuliano et al. 2018). Influenza epidemic patterns differ among temperate, subtropical and tropical regions (Saha et al. 2016). In temperate regions, influenza epi-demics typically occur during the winter months (Finkel-man et al. 2007; Tamerius et al. 2013), such as from November to March in the Northern Hemisphere and from April to September in the Southern Hemisphere, whereas in subtropical and tropical regions, influenza activity occur year-round or one or two peaks per year (Viboud et al. 2006; Moura 2010).
Influenza in Myanmar shows seasonality, and the peak of influenza appears in the rainy season from June to September (Dapat et al. 2009; Htwe et al. 2019). Similarly, influenza in most American tropical regions occurs between April and September (Durand et al. 2016). The positivity rate and number of cases of influenza A in Ethiopia exhibits seasonality, with the peak occurring in November and December (Woyessa et al. 2018). Several Asian countries near the equator, such as Indonesia, Malaysia, Singapore and Vietnam, have identifiable year-round activity (Saha et al. 2014). Some researches in Hong Kong also find that influenza epidemics can occur at any time of the year (Wong et al. 2004; Yang et al. 2015), and the anti-phase patterns between influenza A/H1N1 and A/H3N2 were found in Hong Kong (Chiu APY et al. 2018). Influenza activity appears to coincide with the rainy season in some tropical countries (Shek and Lee 2003; Russell et al. 2008), whereas influenza activity occurs year-round without well-defined influenza seasons (Tamerius et al. 2013).
Macau is one such area that geographically sited in tropics and has a subtropical climate. Macau is located on the south coast of China, with a population density of 20,500 per square kilometer, making it the most densely populated area in the world. Macau is an export-oriented economy and world-famous tourist city with annual tourist traffic exceeds 35 million. The large influx of visitors can increase the complexity of virus types and further facilitate transmission of viruses. In addition, the free vaccination for all people has been conducted in Macau to prevent the influenza. The Health Bureau ordered a total of 190,000 doses of the 2019–2020 quadrivalent influenza vaccine which will provide to people for free. Thus, these unique features should lead to unique research attention to the epidemiological characteristics of influenza in Macau, which should bring great value for preventing influenza in tourist cities in the world. So far, there has been no study published on the epidemiology of influenza in Macau. Therefore, we conducted this study to explore the epi-demiological characteristics of influenza in Macau.
We collected and analysed influenza data from outpa-tients with influenza-like illness (ILI) at Kiang Wu Hospital in Macau from 2010 to 2018. The annual distri-bution of influenza A and B were determined. Three spe-cial influenza epidemics were found. Influenza data among different ages, genders, areas and seasons were calculated and compared. Our study can provide understanding on the epidemiological characteristics of influenza in Macau. The findings could help the prevention of influenza in Macau and over the world.
-
Our study was conducted at Kiang Wu Hospital in Macau from January 2010 to December 2018. Patients were enrolled when they presented with symptoms of influenza-like illness. The criteria for influenza-like illness was a sudden onset of spontaneous fever accompanied by at least one respiratory symptom (cough, sore throat, or running or congested nose) and one systemic symptom (headache, muscle ache, sweats or chills, or tiredness) (Butler et al. 2020). We enrolled a total of 104,874 outpatients with influenza-like symptoms and collected their throat and/or nasal swabs to test the influenza type using the BD Veritor System for rapid detection of Flu A+ B reagent. Results were presented on a standard reporting format. Patients' demographic information, including age, gender and place of residence were recorded.
-
We calculated and compared every year and month posi-tive rate of influenza A and B to reflect annual and monthly distribution. In addition, influenza data were categorized based on the patients' demographic information: age, gender, area and season. The effect of patient age was evaluated by considering the following age groups; 0–4, 5–10, 11–17, 18–39, 40–64 and over 64 years old (Brownstein et al. 2005). The area was classified by locals and tourists. The influenza A in July 2017 and influenza B in January–February 2012 and January–February 2018 were analyzed separately due to their specificity.
The influenza data was summarized by ratios and per-centages. Chi-square test was used to assess the signifi-cance of the association between variables and influenza infection. Binary multivariable logistics regression (Wagner et al. 2017) was conducted to assess potential risk factors associated with infection of influenza A and B. Binary multivariable logistics regression included age, gender, area and season. Odds ratio (OR) was obtained from the logistic regression model and indicated the strength of association between risk factors and influenza. In our study, all analyses were conducted in R language (R-3.4.3). Significance was assessed at an a level of 0.05, and precision was evaluated with 95% confidence intervals (95% CI).
Data Collection
Data Analysis
-
From January 2010 to December 2018, 104,874 samples with ILI were collected at Kiang Wu Hospital, Macau. The samples contained 17,973 cases (17.14%) of influenza A and 7274 cases (6.94%) of influenza B. The information of each year samples was shown in Table 1.
Year Samples Influenza (%) Influenza A (%) Influenza B (%) 2010 9368 1695 (18.09) 1203 (12.84) 492 (5.25) 2011 6997 1608 (22.98) 1489 (21.28) 119 (1.70) 2012 13,054 3674 (28.14) 2209 (16.92) 1465(11.22) 2013 6543 1178 (18.00) 1096 (16.75) 82 (1.25) 2014 8833 2504 (28.35) 2037 (23.06) 467 (5.29) 2015 11,427 2826 (24.73) 2124 (18.59) 702 (6.14) 2016 12,563 2880 (22.92) 1740 (13.85) 1140(9.07) 2017 15,828 4122 (26.04) 3693 (23.33) 429 (2.71) 2018 20,261 4760 (23.49) 2382 (11.76) 2378(11.74) Total 104,874 25,247 (24.07) 17,973 (17.14) 7274(6.94) Table 1. Annual distribution of influenza cases at Kiang Wu Hospital in Macau, 2010–2018.
The number of ILI samples were increasingly collected and the number of samples in 2018 was twice as many as in 2010 (9368 cases in 2010 and 20,261 cases in 2018). The positive rate of influenza was relatively stable in these years, ranging from 18% to 28%. The positive rate of influenza A ranged from 10% to 25% and the positive rate of influenza B ranged from 1% to 10%. In most years, the positive rate of influenza A was greater than influenza B. However, influenza B showed unique activity in 2012 and 2018. The ILI sample number and positive rate in 2012 and 2018 (11.22% in 2012 and 11.74% in 2018) were higher than that in remaining years.
The total number and the mean month positive rate of influenza A and B were showed in Fig. 1 to explore the seasonality of the influenza epidemic. The positive rates in 2012, 2017 and 2018 were different from the remaining years. Note, for convenience of description, we denote the years except these three years as the normal years. First, the positive rate of influenza A in July 2017 was higher ([ 40%) than in the normal years. In addition, the peaks of the influenza B in 2012 and 2018 appeared in January and February with the positive rate (close to 30%) was higher than that in the normal years. In the normal years, the incidence of influenza A occurred year-round and did not show seasonality (Fig. 1A). The positive rates of influenza A in January and February were slightly higher than other months (Fig. 1B). Influenza B showed seasonality with the peak appeared in spring (March to May) (Fig. 1C). The positive rates of influenza B in other months were very low (Fig. 1D).
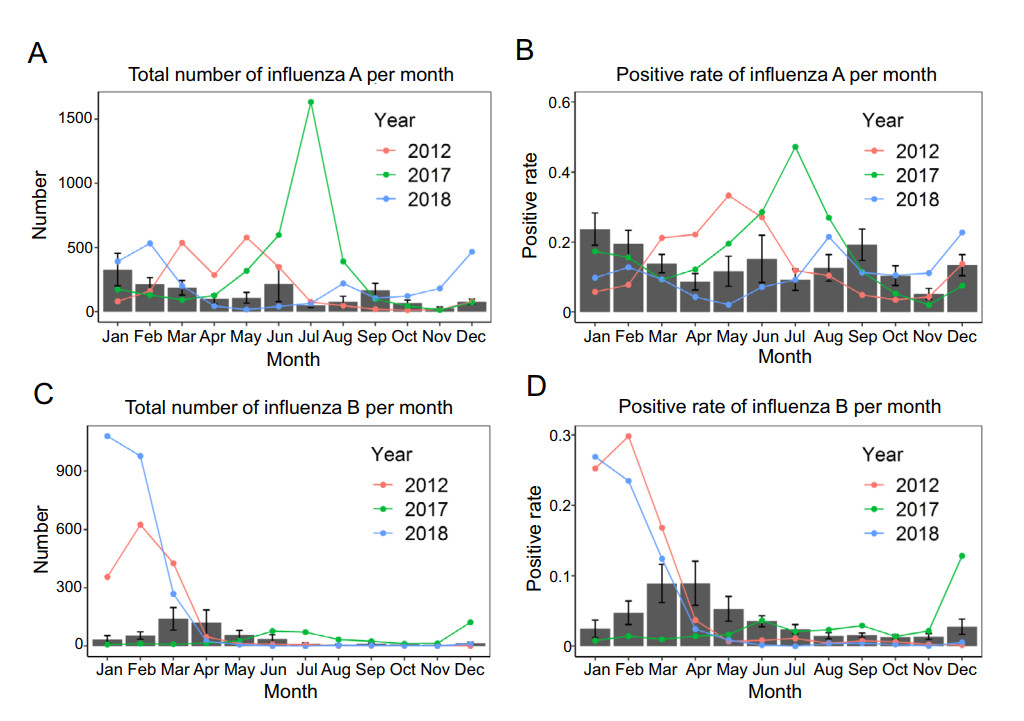
Figure 1. Distribution of influenza A and influenza B. A Total number of influenza A per month. Positive rate of influenza A per month. B Positive rate of influenza A per month. C Total number of influenza B per month. D Positive rate of influenza B per month. The histograms represent the mean number or mean positive rate in the normal years (2010–2011 and 2013–2016). The error bars represent the standard error. The red, green and blue lines represent the trend of influenza A or influenza B in 2012, 2017 and 2018, respectively.
-
The influenza data in the normal years, including 2010–2011 and 2013–2016, were analyzed. A total of 55,731 ILI samples were included, of which 9689 (17.39%) cases were influenza A and 3002 (5.39%) cases were influenza B. The influenza data were classified by age (0–4, 5–10, 11–17, 18–39, 40–64 and > 64 years), gender (fe-male and male), area (local and tourist), and season (spring, summer, autumn and winter). Figure 2 showed the distri-bution of classified influenza data. Table 2 showed the results of univariate analysis, i.e. Chi-square test.
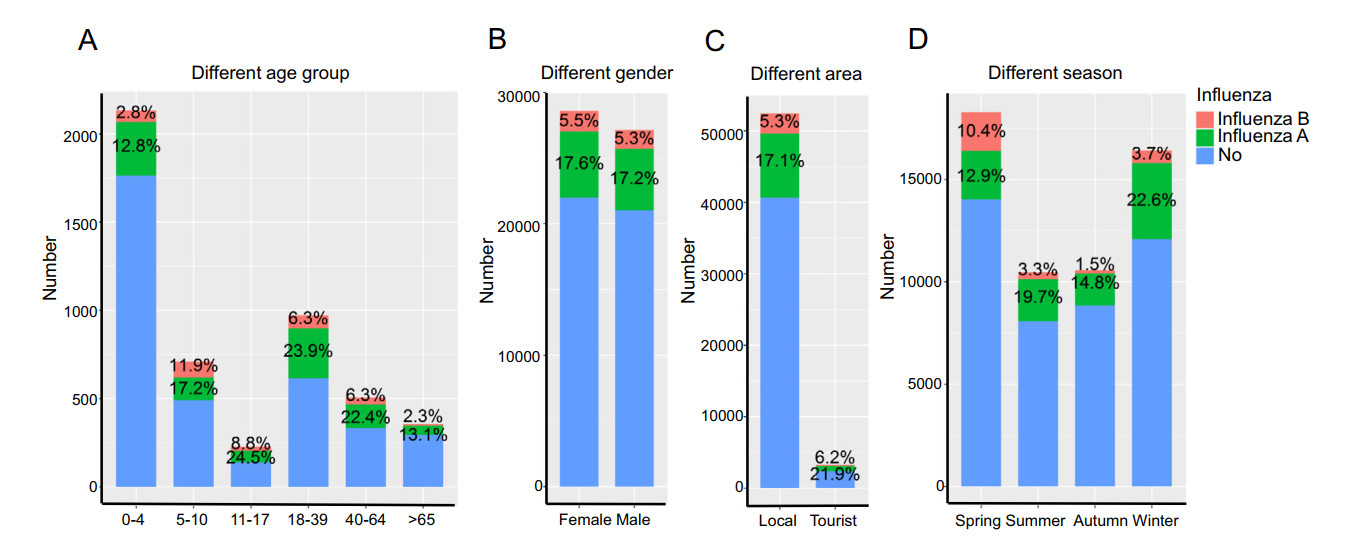
Figure 2. Distribution of influenza A and influenza B among different age, gender, area and season in the normal years. A The number and positive rate of influenza A and B in different age groups. B The number and positive rate of influenza A and B in different genders. C The number and positive rate of influenza A and B in different areas. D The number and positive rate of influenza A and B in different seasons.
Variable Samples Influenza A Influenza B Number (%) Chi-square Number (%) Chi-square Age 0–4 23,710 3039 (12.82) χ2 = 949.75 658(2.78) χ2 = 1110.6 5–10 7492 1288 (17.19) P < 2× 10-16 894(11.93) P < 2× 10-16 11–17 2696 660 (24.48) 236(8.75) 18–39 11,798 2824 (23.94) 741(6.28) 40–64 6036 1354 (22.43) 381(6.31) > 64 3999 524 (13.10) 92 (2.30) Gender Female 28,590 5029 (17.59) χ2 = 1.68 1559 (5.45) χ2 = 0.48 Male 27,141 4660 (17.17) P = 0.1943 1443 (5.32) P = 0.488 Area Local 52,439 8968 (17.10) χ2 = 49.35 2797 (5.33) χ2 = 4.68 Tourist 3292 721 (21.90) P < 2× 10-12 205(6.23) P = 0.0306 Season Spring 18,288 2357 (12.89) χ2 = 653.94 1901 (10.39) χ2 = 1406.5 Summer 10,468 2059 (19.67) P < 2× 10-16 341(3.26) P < 2× 10-16 Autumn 10,568 1566 (14.82) 153(1.45) Winter 16,407 3707 (22.59) 607(3.70) Table 2. Chi-square test results of influenza A and B by age, gender, area, and season in normal years.
The number of ILI samples aged 0–4 years old was the highest among all age groups, accounting for 42.5% of the total. Children were thus the most prone to ILI symptoms and were willing to go to the hospital for diagnosis and treatment. The positive rate of influenza A and influenza B in 0–4 year-old group (influenza A: 12.8%; influenza B: 2.8%) and the > 64 year-old group (influenza A: 13.2%; influenza B: 2.3%) were low compare to other age groups (Fig. 2A). The positive rate of influenza A was highest in 18–39 year-old group (23.9%), while the positive rate of influenza B was highest in 5–10 year-old group (11.5%). The results of Chi-square test proved that the difference among different age groups was significant (influenza A: P < 2× 10-16; influenza B: P < 2× 10-16).
ILI samples were classified by gender (28,590 females and 27,141 males). We calculated and compared the pos-itive rate of influenza A and influenza B in female and male. The positive rates of influenza A and B in females were slightly higher than those in males (influenza A: 17.59% for female and 17.17% for male; influenza B: 5.45% for female and 5.32% for male) (Fig. 2B). The Chi-square test indicate no significant difference between females and males (influenza A: P = 0.1943; influenza B: P = 0.488).
We divided ILI samples into local and tourists. The positive rates of influenza A and B among tourists were higher than that among locals (influenza A: 17.10% for local vs 21.90% for tourist; influenza B: 5.33% for local vs 6.23% for tourist) (Fig. 2C). The Chi-square test proved that the difference was significant between local and tourist (influenza A: P < 2× 10-12; influenza B: P = 0.0306).
The epidemic of influenza also varied season by season. ILI samples were mostly collected during spring and winter. The positive rate of influenza A was the highest in winter (22.6%) and the lowest in spring (12.9%) (Fig. 2D). But the positive rate of influenza B was the highest in spring (10.4%). The results of Chi-square test proved that the difference among different season is significant (in-fluenza A: P < 2× 10-16; influenza B: P < 2× 10-16).
Binary multivariable logistic regression was used to explore risk factors associated with influenza A and B. The variables include age, gender, area and season. The forest plot of logistic regression was showed in Fig. 3A, 3B and the detailed values of logistic regression were shown in Supplementary Table S1. First, for different age groups, the odds of influenza A and B were lower in the 0–4 year-old group and > 64 year-old group than other age group. The odds of influenza A in the 11–17 years-old group were twice as that in the 0–4 year-old group (OR = 2.21, P < 2× 10-16). The 11–17 year old group showed the highest odds of influenza A. The odds of influenza B in the 5–10 year-old group were 4 times higher than the odds in 0–4 year-old group (OR = 4.38, P < 2× 10-16). The 5–10 year-old group had the highest odds of influenza B. Secondly, consistent with the results of Chi-square test, the results of binary multivariable logistic regression showed that no significant difference in infections of influenza A and B between female and male. Thirdly, although the odds of influenza A and B in tourist was slightly higher than that in locals (influenza A: OR = 1.09, P = 0.0557; influenza B: OR = 1.15, P = 0.0771), the difference was not signif-icant. The result is not the same as the result of the Chi-square test. The reason for this phenomenon is that the covariate affects the result of multiple logistic regression (Wang et al. 2017). Area was not a risk factor for infection of influenza A and B in the normal years. Finally, the odds of influenza A were the lowest in spring, while the odds of influenza B were the highest in spring.
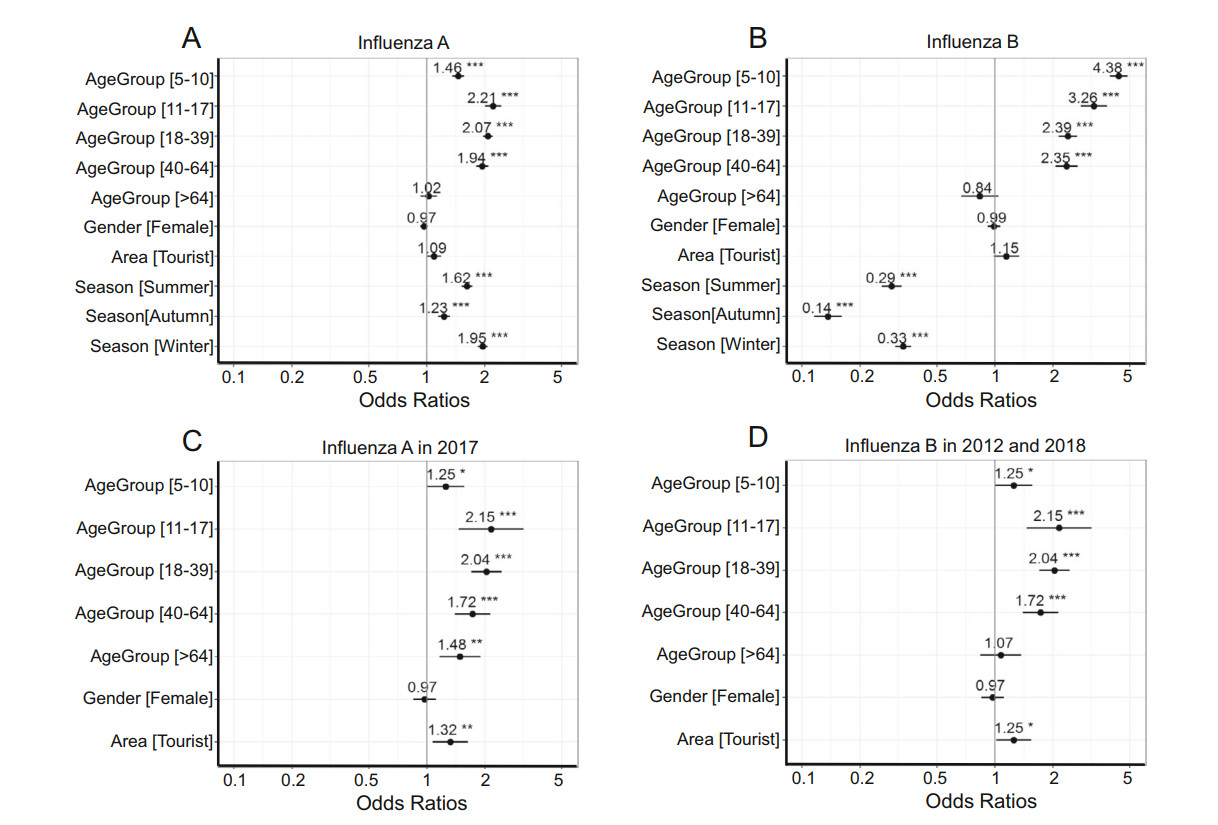
Figure 3. Forest plot of binary multivariable logistic regression. A Binary multivariable logistic regression of influenza A in normal years. B Binary multivariable logistic regression of influenza B in normal years. C Binary multivariable logistic regression of influenza A in July 2017. D Binary multivariable logistic regression of influenza B in January–February 2012 and January–February 2018. The asterisk represents the significance level (*** < 0.001, ** < 0.01, * < 0.05).
-
Because the epidemic of influenza A in July 2017 is dif-ferent from the normal years, we extracted influenza A data in July 2017 and compared it with the data in July of normal years. The distribution of influenza A and the comparison between 2017 and normal years were showed in Table 3. A total of 3461 ILI samples were collected in July 2017, which exceeded the total samples of the normal years (2577 samples in six years). Also, the positive rate of influenza A in July 2017 was 47.2%, which was signifi-cantly higher than that (11.6%) in July of normal years (P < 2× 10-16). The forest plot of logistic regression was showed in Fig. 3C and the detailed values of logistic regression were shown in Supplementary Table S2.
Variables Influenza A in 2017 Influenza A in normal P value Samples N (%) P value Samples N (%) Age 0–4 1335 519 (38.9) χ2 = 80.43 1109 83(7.5) < 2× 10-16 5–10 419 188 (44.9) P =7910-16 269 28(10.4) < 2× 10-16 11–17 116 68 (58.6) 116 14(12.1) 3× 10-13 18–39 789 449 (56.9) 549 99(18.0) < 2× 10-16 40–64 478 253 (52.9) 288 45(15.6) < 2× 10-16 > 64 324 157 (48.5) 246 30(12.2) < 2× 10-16 Gender Male 1679 784 (46.7) χ2 = 0.31 1289 152 (11.8) < 2× 10-16 Female 1782 850 (47.7) P = 0.5771 1288 147 (11.4) < 2× 10-16 Area Local 3042 1401 (46.1) χ2 = 13.11 2414 273 (11.3) < 2× 10-16 Tourist 419 233 (55.6) P < 0.0003 163 26(15.9) < 2× 10-16 Total 3461 1634 (47.2) 2577 299 (11.6) < 2× 10-16 Table 3. Distribution and comparison of influenza A in July 2017.
The Chi-square test and logistic regression show sig-nificant differences among different age groups. The odds of influenza A in the 11–17 year-old group (OR = 2.15, P-value = 0.0001) and 18–39 year-old group (OR = 2.04, P value = 1.29× 10-14) were twice as the odds of influ-enza A in 0–4 year-old group.
Consistent with the results in the normal years, the results of Chi-square test and logistic regression indicated there is no significant difference between male and female (P = 0.5771). However, the differences in influenza A infection between locals and tourists is significant. The odds of influenza A in tourists (OR = 1.32, P value = 0.0091) were significantly higher than local.
-
Because the epidemic of influenza B in January–February 2012 and January–February 2018 is different from the normal years, we extracted influenza B data in this period and compared it with the influenza B in January–February of normal years. The distribution of influenza B and the comparison between 2012, 2018 and normal years were showed in Table 4. A total of 11,677 ILI samples were collected in January–February 2012 and January–February 2018, which was close to the total samples of the normal years (13,206 samples in six years). Also, the positive rate of influenza B in January–February 2012 and January– February 2018 was 25.9%, which was significantly higher than that (3.9%) in January–February of normal years (P < 2× 10-16). The forest plot of logistic regression was showed in Fig. 3D and the detailed values of logistic regression were shown in Supplementary Table S2.
Variables Influenza B in 2012 and 2018 Influenza B in normal Chi-Squre Samples N (%) P value Samples N (%) Age 0–4 4369 675 (15.4) χ2 = 566.35 5338 125 (2.3) < 2× 10-16 5–10 2362 926 (39.2) P < 2× 10-16 1561 129 (8.3) < 2× 10-16 11–17 647 260 (40.2) 667 32 (4.8) < 2× 10-16 18–39 2435 714 (29.3) 3302 138 (4.2) < 2× 10-16 40–64 1275 349 (27.4) 1494 79 (5.3) < 2× 10-16 > 64 589 110 (18.7) 824 15 (1.8) < 2× 10-16 Gender Male 5498 1384 (25.2) χ2 = 3.11 6321 235 (3.7) < 2× 10-16 Female 6188 1650 (26.7) P = 0.0779 6885 283 (4.1) < 2× 10-16 Area Local 10,486 2681 (25.6) χ2 = 9.01 12,284 464 (3.8) < 2× 10-16 Tourist 1191 353 (29.6) P = 0.0027 922 54 (5.9) < 2× 10-16 Total 11,677 3034 (25.9) 13,206 518 (3.9) < 2× 10-16 Table 4. Distribution and comparison of influenza B in January–February 2012 and January–February 2018.
Among different age groups, the odds of influenza B were the highest in the 5–10 year-old group (OR = 3.51, P < 2× 10-16) and 11–17 year-old group (OR = 3.66, P < 2× 10-16), and lowest in 0–4 year-old group and > 64 year-old group (OR = 1.07, P = 0.3131).
Consistent with the results in the normal years, the Chi-square test and logistic regression result showed no sig-nificant differences in infections of influenza B between male (OR = 1.03, P value = 0.4670) and female. However, the differences in influenza B infection between locals and tourists were significant. The odds of influenza B in tourists (OR = 1.25, P value = 0.0474) were significantly higher than local.
Influenza Changes Over the Years and Months
Epidemiology of Influenza in the Normal Years
Influenza A Epidemic in 2017
Influenza B Epidemic in 2012 and 2018
-
To investigate the epidemiological characteristics of influenza, we examined 104,874 samples with ILI in Macau from 2010 to 2018. This is the first time that the epidemiological characteristics of influenza are examined in Macau. Based on our analysis on these samples, we have the following findings. First, our results show that, among these ILI samples, the overall positive rate is 17.17% for influenza A and 6.97% for influenza B (Table 1). However, the influenza epidemics in three special years (i.e., 2012, 2017 and 2018) differed from the remaining years (i.e., normal years). The positive rate of influenza A in July 2017 (47.2%) was significantly higher than that in July of normal years (11.6%) and the positive rate of influenza B in Jan-uary–February 2012 and January–February 2018 (25.9%) was significantly higher than that in January–February of normal years (3.9%). Second, in a normal year, influenza A did not show obvious seasonality, while influenza B was seasonal in Macau. Third, the odds of influenza A and B were lower in children (0–4 years old) and elderly (> 64 years old) than the four other age groups (5–10, 11–17, 18–39, 40–64 years old), but the difference of influenza A and B infection between male and female was not significant (Fig. 3). Finally, our analysis showed that in a normal year, there was no significant difference between locals and tourists in influenza A and B infection. How-ever, in July 2017, the odds of influenza A in tourists were significantly higher than those in locals (OR = 1.32, P value = 0.0091) (Supplementary Table S2); in January– February 2012 and January–February 2018, the odds of influenza B in tourists were significantly higher than those in locals (OR = 1.25, P value = 0.0474) (Supplementary Table S2). We give discussions on these findings below.
Our results show that the overall positive rate is 17.17% for influenza A and 6.97% for influenza B. The positive rate of influenza in Macau is much lower than that in Myammar from 2010 to 2015 (influenza A: 55.1%; influ-enza B: 28.3%) (Htwe et al. 2019), and also lower than or close to the positive rate of influenza in Ethiopia from 2009 to 2015 (20.6%) (Woyessa et al. 2018) and in tropical Asia from 2007 to 2013 (South China: 17.3%; Thailand: 18%; Philippines: 17.2%; Singapore: 24.6%) (Durand et al. 2016). It indicates that the influenza in Macau is well controlled although Macau is a city with the highest pop-ulation density and a large population mobility. Our results also show that the number and positive rate of influenza A were generally higher than those of influenza B. Influenza A viruses were predominant in most of the season; influ-enza B viruses predominated in spring (March to May) (Fig. 1). The trend and peak of influenza A and B in USA (Blanton et al. 2017; Garten et al. 2018; Xu et al. 2019) is similar to that in Macau.
Our analysis shows an age effect. That is, the odds of influenza A and B were lower in the children and elderly than the four other age groups in Macau. The similar age effect is also reported in Ethiopia (Woyessa et al. 2018). There may be the following three reasons about this age effect. First, as a common belief, influenza can cause more damage to the health of the children and elderly. Thus, these two age groups are more likely to get vaccination than the other four age groups, leading to a better pre-vention of influenza that resulted in a lower odd of influ-enza in the children and elderly. Second, children and elderly cannot express their symptoms very clear. Thus, some of them with mild influenza symptoms will also be considered as ILI samples. The inclusion of these samples increases the total number of samples, but the number of influenza cases remains unchanged, so the positive rate in children and elderly is low.
Our results show that Macau experienced a special epidemic of influenza A in the summer season of 2017 and two special epidemic of influenza B in January–February 2012 and January–February 2018. The number and positive rate of influenza A or influenza B were significantly higher in these special years than that in normal years either in tourists or in locals. The epidemic of influenza A similar to what it is in Taiwan and Hong Kong because the influenza season in Taiwan and Hong Kong in 2016 and 2017 also showed an unusual summer peak mainly due to the spread of influenza A (H3N2) virus (Tsou et al. 2017; Chiu SS et al. 2018). The epidemic of influenza B in January– February 2012 and January–February 2018 in Macau coincided with the influenza B epidemic in mainland China. During the winter season of 2012–2013 and 2017–2018, China experienced a nationwide influenza epidemic mainly caused by influenza B virus which belonged to the Yamagata lineage (Radovanov et al. 2015; Saha et al. 2016; Li et al. 2019; Zhu et al. 2019). This phenomenon shows that three special influenza epidemics in Macau is closely related to its neighboring areas. The mobility of tourists has caused the virus to spread to locals, thus increasing the numbers and positive rates of influenza in locals.
One important finding in our study is that, there is no significant difference between locals and tourists in influenza A and B infection in a normal year (Fig. 3A, 3B) whereas the odds of influenza A in tourists were significantly higher than those in locals in July 2017 (Fig. 3C) and the odds of influ-enza B in tourists were significantly higher than those in locals in January–February 2012 and January–February 2018 (Fig. 3D). This finding further revealed that the epi-demic of influenza in Macau is affected by the mobility of tourists. Moreover, Macau government provides free seasonal influenza vaccination to all permanent residents. The free vaccination starts around October each year and is provided to high-risk groups first. Then, around December, the free vaccination is extended to all residents. A survey revealed that the estimated proportion of the total population covered by the number of vaccines purchased in Macau is 19.8% in 2011, which is higher than its neighboring areas (6.8% in Hong Kong) (Dwyer et al. 2013). With the further implementation of government propaganda work, the dose of vaccine purchased by the government is increasing (110,000 doses in 2011 vs 190,000 doses in 2019), and the number of residents receiving influenza vaccine is increasing (about 85,000 in 2011 vs about 160,000 in 2019). The vaccination rate is over 80% for kindergarten children, over 70% for primary school students and almost 40% for elderly. Therefore, compared with tourists, the higher vaccination rate of locals can effectively reduce the incidence of influ-enza among locals. This may also support that vaccination is an important way to prevent influenza.
The influenza data in Macau could contribute to study on the circulation pattern of influenza and help the pre-vention of influenza not only in Macau but also in Hong Kong, Taiwan and other regions in the world. Our epi-demiological study on influenza A and B could be helpful to prevent influenza in Macau and provide guidance on vaccine strain selection and adjustment of time for vacci-nation. Vaccination is the most effective approach to reduce the prevalence of influenza (Rolfes et al. 2019; Sah et al. 2019). Although Macau is a city with a high density and a large mobility of population, the influenza in Macau is well controlled, which is attributed to the employment of free vaccination for all people in Macau. Therefore, we hope that free vaccination could be employed in more regions in the future.
In sum, we analyzed the epidemiological characteristics of influenza A and B in Macau and found that influenza in Macau has been well controlled, which may benefit from the implementation of free vaccination for all people in Macau. Further studies are needed to explore the contribution of vaccine teammates to control influenza in Macau in combi-nation with detailed influenza vaccination data in Macau.
-
This work was supported by the University of Macau (Grant Numbers: FHS-CRDA-029-002-2017, EF005/FHS-ZXH/2018/GSTIC and MYRG2018-00071-FHS) and by the Science and Technology Development Fund, Macau SAR (File No. 0004/2019/AFJ).
-
XDZ and JLN conceived the study with input from all co-authors. HMN, SMK, MIW, CHW and JLN collected the data. TZ, GLW, GYM, ZL, CC and DDW did the data analyses and HMN, TZ, XDZ and JLN performed the interpretation of the data. HMN and TZ wrote the first draft of the manuscript, and XDZ revised and approved the final manuscript. All authors contributed to the final version and agreed to the submission.
-
The authors have declared that no competing interest exists.
-
This study was conducted with the approval of the Animal Ethics Committee of Kiang Wu Hospital in Macau.

 DownLoad:
DownLoad: