Influenza is one of the oldest infectious diseases affecting humans. Every influenza pandemic in history has ended with disastrous outcomes regarding public health and the social economy. November 1, 2018, marked the first “World Flu Day” that was formally launched at the Asian-Pacific Centenary Spanish 1918-Flu Symposium in Shenzhen, China. The campaign was initiated and developed by Dr. George F. Gao in collaboration with other world’s leading influenza specialists. The “World Flu Day” initiative aimed to raise public awareness about influenza, to accelerate scientific innovation and international cooperation on influenza surveillance, and to push for stronger global support on influenza prevention and control. The sculpture entitled “Quarere Veritatem” in the cover represents an influenza virus.
Influenza is one of the oldest infectious diseases affecting humans. Every influenza pandemic in history has ended with disastrous outcomes regarding public health and the social economy. This year marks the 100th anniversary of the Spanish flu (H1N1) outbreak of 1918, which is recognized as the most lethal natural event in recent history. In spite of limited travel and transportation at that time, the Spanish flu pandemic of 1918 reached peak activity on multiple continents simultaneously within several months after its emergence in late 1917 from different hypothesized origins, such as US military camps, the state of Kansas, or the troop staging and hospital camp in Éxtaples, France (Patterson and Pyle 1991; Oxford et al. 2005; Shanks 2016). However, in some islands of the Pacific region, such as in New Caledonia, the pandemic's lethal effects lasted for over 3 years, until July 1921 (Shanks et al. 2018). The pandemic flu is estimated to have infected more than 500 million people, causing between 50 and 100 million deaths globally (Patterson and Pyle 1991; Guan et al. 2010). The evidence suggests that most pandemicrelated deaths were not caused by the direct pathological effects of the influenza virus, but rather by the lethal effects of secondary bacterial pneumonia (Chien et al. 2009).
The 2018 Medicine Nobel Prize was awarded jointly to two immunologists, James P. Allison at the University of Texas MD Anderson Cancer Center in Houston and Tasuku Honjo at Kyoto University in Japan, who pioneered a new way to treat cancers (Ledford et al. 2018). Both Laureates have shown how so called "immune checkpoints" on T cells can be used to manipulate the immune responses so that T cells can efficiently attack cancer cells. Using the immune system to fight cancers has been investigated for more than a 100 years. Recent advances in cancer immunotherapy, particularly immune checkpoint blockade therapy have dramatically changed the therapeutic strategy against advanced cancers. Through inhibiting negative immune regulation, these approaches have demonstrated improved overall survival for patients with advanced cancers. Importantly, for some of the patients treated with such strategies, their tumors seem to totally disappear.
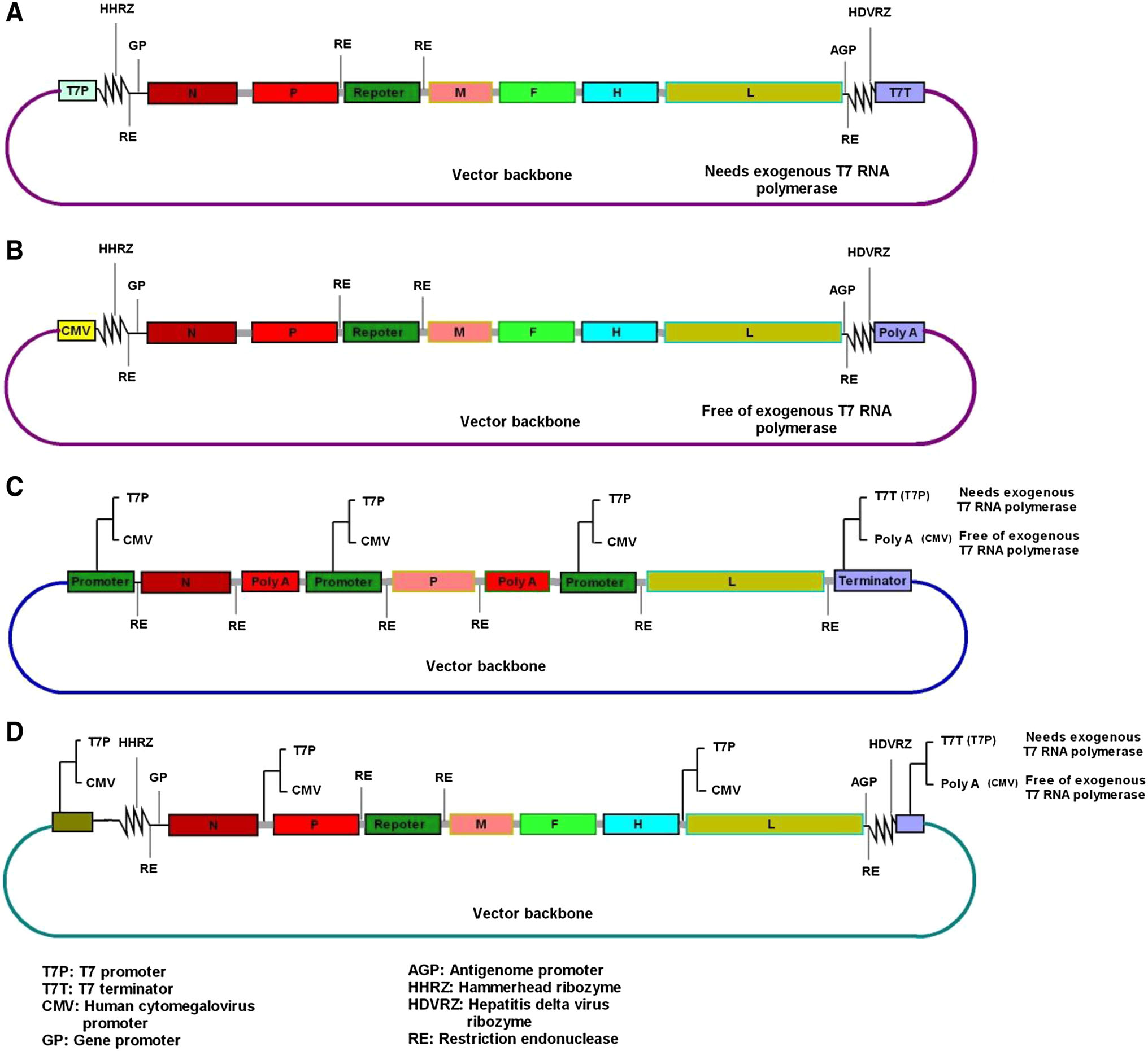
Peste des petits ruminants (PPR) is a highly contagious transboundary animal disease with a severe socio-economic impact on the livestock industry, particularly in poor countries where it is endemic. Full understanding of PPR virus (PPRV) pathobiology and molecular biology is critical for effective control and eradication of the disease. To achieve these goals, establishment of stable reverse genetics systems for PPRV would play a key role. Unfortunately, this powerful technology remains less accessible and poorly documented for PPRV. In this review, we discussed the current status of PPRV reverse genetics as well as the recent innovations and advances in the reverse genetics of other non-segmented negative-sense RNA viruses that could be applicable to PPRV. These strategies may contribute to the improvement of existing techniques and/or the development of new reverse genetics systems for PPRV.
We describe the first genome isolation of Middle East respiratory syndrome coronavirus (MERS-CoV) in Kenya. This fatal zoonotic pathogen was first described in the Kingdom of Saudi Arabia in 2012. Epidemiological and molecular evidence revealed zoonotic transmission from camels to humans and between humans. Currently, MERS-CoV is classified by the WHO as having high pandemic potential requiring greater surveillance. Previous studies of MERS-CoV in Kenya mainly focused on site-specific and archived camel and human serum samples for antibodies. We conducted active nationwide cross-sectional surveillance of camels and humans in Kenya, targeting both nasal swabs and plasma samples from 1, 163 camels and 486 humans collected from January 2016 to June 2018. A total of 792 camel plasma samples were positive by ELISA. Seroprevalence increased with age, and the highest prevalence was observed in adult camels (82.37%, 95% confidence interval (CI) 79.50-84.91). More female camels were significantly seropositive (74.28%, 95% CI 71.14-77.19) than male camels (P < 0.001) (53.74%, 95% CI 48.48-58.90). Only 11 camel nasal swabs were positive for MERS-CoV by reverse transcription-quantitative PCR. Phylogenetic analysis of whole genome sequences showed that Kenyan MERS-CoV clustered within sub-clade C2, which is associated with the African clade, but did not contain signature deletions of orf4b in African viruses. None of the human plasma screened contained neutralizing antibodies against MERS-CoV. This study confirms the geographically widespread occurrence of MERS-CoV in Kenyan camels. Further one-health surveillance approaches in camels, wildlife, and human populations are needed.